GOLFER’S ELBOW/MEDIAL EPICONDYLITIS
Introduction
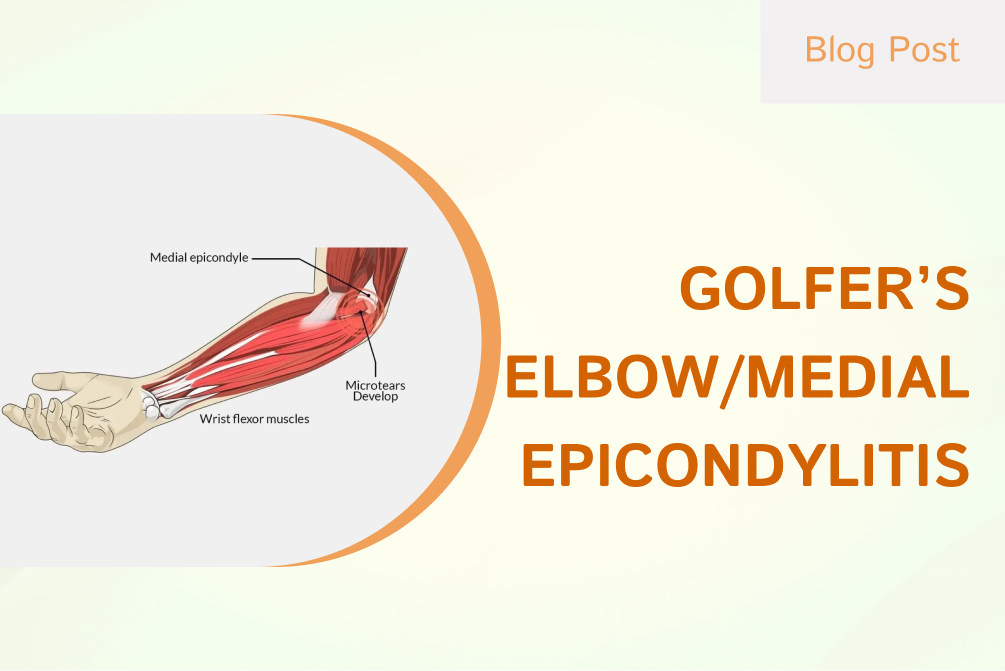
Medial epicondylitis, or more commonly known as golfer’s elbow is a tendonitis/tendinopathy of the common flexor tendon which sits on the inside part (medial) of your elbow. This is often caused by repetitive stress activities that overload the common flexor tendon Golfers account for a significant portion of sports-related cases among these, with the usual suspects being those involving an overhead throwing activity. The medial epicondyle is where the bony humeral ulnar-sided attachment for muscles of the common flexor tendon occurs.
COMMON TERMINOLOGIES
- Medial Epicondylitis
- Medial Epicondylalgia
- Golfer’s elbow
- Pitcher’s Elbow
- Common Flexor Tendon of Elbow tendinosis/tendinopathy
ETIOPATHOGENESIS
Symptoms could be triggered by hand and arm movements (including the wrist), such as grasping, lifting, twisting, or bending. Golfer’s elbow tends to happen within people who engage in an activity where the flexor muscles are overworked which they are generally not used to or if you use your demands daily repetitive strain of the flexor muscle. The term golfer’s elbow is a bit of a misnomer as medial epicondylitis much more often occurs with other overuse activities.
The most accepted theory is that repetitive loading of the common flexor muscles causes micro-tears at the tendinous origin, triggering an inflammatory response. In chronic Tendinosis, the remodeling of the collagen fibers results in a thickening tendon as it progresses. Calcification may also occur with it.
The likely causes may be
- Occupations demanding manual labour such as wood chopping, repairing automobiles, painting and hammering can produce repetitive load on the flexor muscles.
- Sporting activities such as golf, weightlifting or sports involving overhead throwing actions like javelin and short put can lead to medial epicondylitis.
- Working at a computer for long hours.
- Cooking involving regular chopping and peeling.
PREVALENCE
Golfer’s Elbow occurs in not more than 1% of the population. Being predominantly noted in patients of 40–60 years. Its counterpart Tennis Elbow (lateral epicondylitis) is known to be very common in the community. Preponderance is equally balanced in men and women.
SYMPTOMS
The usual complaint from patients is dull aching pain on the medial/inner side of the elbow. Epicondylitis pain radiates down to the forearm and wrist from a bony prominence (medial epicondyle).
Such activities like writing and lifting which require the wrist to be bent may worsen pain. The symptoms are likely to be aggravated while making sudden jerky movements as can occur in golf or overhead throwing games, etc.
Some patients may have difficulties grabbing objects and others with more severe symptoms could even report a slight decrease in their grip strength. Rest often settles the symptoms but there may be residual achiness that does not allow for sleep either, and concerns patients with potential ulnar nerve involvement
Ulnar nerve involvement may be additional in up to 20% of patients. Symptoms often include numbness and tingling over the ulnar nerve distribution down to 5th followed by a hand condition shown secondary in weakness/stiff elbow accessed.
CLINICAL EXAMINATION
A patient may appear unwell with acute swelling, redness, and warmth; in chronic cases, this symptom complex is less often encountered. Pain is commonly elicited by palpation just anterior and distal to the medial epicondyle.
There are two parts to the clinical testing for golfer’s elbow / medial epicondylitis; an active and a passive component.
For the active component, the patient should resist wrist flexion with the arm in extension and supination. For Passive Component Wrist Extension with Elbow in Extension. If these provocative maneuvers produce pain, the golfer’s elbow should feature highly in the clinical differential diagnosis. Clinical assessment must incorporate ruling out ulnar neuropathy
There may be erythema, swelling, or warmth on the exam in acute cases; chronic events have less chance of revealing any abnormalities. Localization tenderness will be at the site or 5-10 mm distal and anterior from it in an area close to the conjoined tendon if not combining both groups
The golfer elbow test / medial epicondylitis test has a passive and an active component. The patient actively resists wrist flexion while the arm is in extension and supination. The passive element involves being in wrist extension with the elbow extended. A positive test is one in which the patient describes pain with this maneuver.
However, the difference is that Tinel‘s test should be used to evaluate for ulnar neuropathy and stress particularly applied to the ulnar collateral ligament in a throwing athlete.
INVESTIGATION
A diligent history and physical exam are typically highly suggestive of the diagnosis, but imaging studies such as musculoskeletal ultrasound or MRI of the elbow may be performed to confirm the findings.
TREATMENT
For most cases of golfer’s elbow, conservative management is recommended. It means: to enforce that constraint as far as possible, particularly within the constraints of an individual’s vocation. Medical management consists of anti-inflammatory medications. Use ice or cold packs when inflammation is at its worst. Modalities like Ultrasound, shock waves, and electrical stimulation have been tried. When it comes to physical therapy, eccentric exercises are key. Right Stretching and strengthening certainly is an integral part of the rehabilitation process. Other patients will be recommended with night splints.
Anti-Inflammatory injection: If a patient is in pain, Corticosteroids can be injected blindly or under image guidance at the inflamed site to take inflammation down so that they may start with their rehabilitation. To avoid such setbacks repeat steroid injections in the same area should be prevented.