Trigeminal neuralgia (TN)
It is characterized by recurrent unilateral short (seconds) electric shock-like facial pain triggered by light stimuli in the trigeminal nerve distribution and is abrupt in onset and termination. Pain is limited to one or more of the trigeminal divisions, and innocuous sensory stimuli evoke it. TN is classified into classical TN (CTN) or secondary TN (STN) due to multiple sclerosis or a space-occupying lesion (e.g. tumor, cerebral aneurism, or megadolicho basilar artery).
Epidemiology
TN is frequently both misdiagnosed and underdiagnosed: Trigeminal neuralgia (TN) is often misdiagnosed, and an equally high percentage of patients are underdiagnosed. The prevalence of TN varies between studies, ranging from 4.3 to 27 new cases per 100,000 persons/year. It is more common in women, and higher with increasing age. In population-based studies, the lifetime prevalence was estimated at 0.16 – 0.3%. The age at onset of Classical TN and Secondary TN are commonly 53 years and 43 years respectively, but can occur from early to old ages. In studies done in the tertiary care setup, STN has been estimated to constitute 14–20% of TN patients.
Etiology and Pathogenesis
As early as 1930, Dandy suggested conservatively that 30% of patients with trigeminal neuralgia had vascular compression of the trigeminal nerve as a cause. Complicated Trigeminal Neuralgia which includes multiple sclerosis and such related conditions may occasionally develop classical-type pain due to a similar mechanism. The current understanding of the mechanism of Classical Trigeminal Neuralgia is that it is either due to compression or morphological changes in the trigeminal nerve due to mainly an artery in the cerebellopontine cistern. This is called a NEUROVASCULAR CONFLICT with compression. However, this also allowed many anatomical specimens to be identified which showed a transition from Schwann cell myelination to oligodendroglia myelination.
TRIGEMINAL NEURALGA (SYNDROME)
This term originated as Tic Doloureux, mindful of the characteristic grimace of TN patients occurring at the time of a painful paroxysm.
Patients described the pain as sharp shooting and stabbing and electric shock-like sensations. Trigeminal Neuralgia: The pain paroxysm of Trigeminal Neuralgia is one of the more painfully debilitating experiences that the system can go through. This type of highly unpleasant pain is terrifying for patients because the onset is sudden and unexpected.
The duration of a Pain Paroxysm varies, from a few seconds to occurring several times per day and these paroxysms are also can be initiated into repeated succession again and again following a refractory period. It can be experienced as a still series of attacks interspersed with many fits, punctuated with close runs. This paroxysmal pain may be associated with background dull achy continuous pain which tends to be milder as compared to paroxysmal pain. This background headache has been attributed more frequently to women.
Refractory period and precipitating factors
A common finding among patients after the paroxysmal attack is that they will not experience another attack during a refractory period (the time after an attack). This phenomenon has been attributed to the hyperpolarisation of the sensory neuron. Several patients go through a refractory period after paroxysmal attack in which no new attacks can be induced. The mechanism behind this phenomenon remains unknown. It was suggested that it is due to hyperpolarisation of the sensory neuron.
Astonishingly, the pain of Trigeminal Neuralgia can be provoked by innocuous sensory stimuli to the affected side of the face. The stimuli can be intraoral or extraoral. Well-known triggers are ordinary daily living such as light touch, speaking, chewing, brushing teeth, and cold wind blowing against the face.
Site of lesion
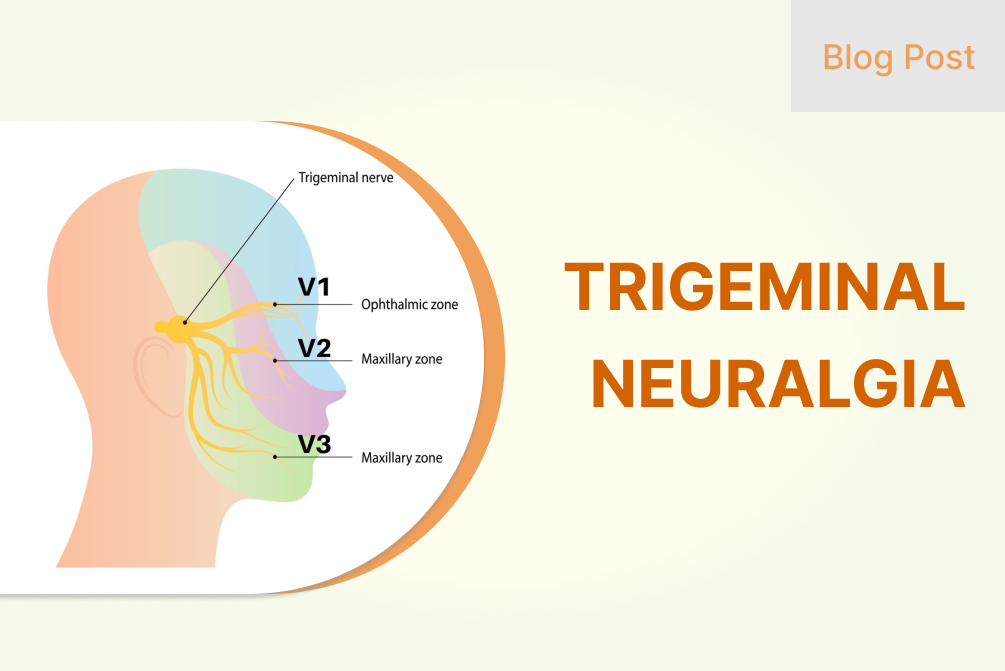
Affected most often are the second and third divisions of the trigeminal nerve. The right side is affected more often. Bilateral TN is uncommon in the classical form and should signal Secondary TN.
Natural Progression
It was previously assumed that TN becomes chronic and that pain gets worse over time. It has been suggested to worsen with time and TN in its chronic form is defined by more persistent, medically refractory pain, sensory abnormalities, and progressive neuroanatomical changes of the trigeminal root. More recently, studies have contested this notion, demonstrating that in most patients the pain did not increase in frequency or duration and did not become resistant to treatment, as well as, the dose limit has remained stable. A further common finding is months and even years of total remission. This is due to a decrease in irritable properties of nerve and partial demyelination.
Facial pain with autonomic symptoms
Tearing and rhinorrhea have long characterized TN. A large percentage of TN patients also consist of autonomic symptoms as a part of the symptom complex. The trigger seems to be the trigemino vascular reflex that is provoked by strong facial pain. Other causes of unilateral primary headache that may present similarly include short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing, and short-lasting unilateral neuralgiform headache attacks with autonomic symptoms.
The diagnosis of TN is essentially historical. Important to the history taking is the onset of the pain. A must be the history of any prior Herpes Zoster rash in that area, any invasive dental treatment, or any significant trauma to the ipsilateral side of the face. In the case of the history of a dental procedure or trauma, the possibility of Post Traumatic Trigeminal Neuropathy (PPTN) PPTN might be similar to TN but is characterized by discrete sensory deficits.
This must be confirmed with a detailed dental checkup to exclude the possibility of a cracked tooth (probably secondary to chewing hard foods) which can mimic the pain of TN. Even when the pain was bilateral constant in the jaw area, the potential for tension-type headache, temporomandibular joint disorder, and persistent idiopathic facial pain might increase.
Other differential diagnoses are Occipital neuralgia, paroxysmal hemicrania, glossopharyngeal neuralgia, short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing, and short-lasting unilateral neuralgiform headache attacks with autonomic symptoms
Magnetic resonance imaging (MRI) imaging is useful for imaging changes in trigeminal root, any neuromuscular compression (e.g., tumors, vascular loops), and secondary pathology, but it is primarily a clinical diagnosis. The nerve can be diagnosed as the entire course of the nerve, root atrophy, and CPA cistern.
Treatment
Trigeminal Neuralgia has failed abortive treatments but still pharmacological management is the mainstay. Only when medical management cannot control the symptoms, ablative and non-ablative interventional procedures are reserved for patients.
CBZ and OXC
Carbamazepine and oxcarbazepine are the first-line management offered to patients suffering from TN. These are considered effective in providing initial pain control in 90% of the patients [35] although these effects may unfortunately fade with chronicity. Due to their severe side effect profile, these drugs are withdrawn in up to 40% of the patients. Women have a lower threshold for these drugs. [36] Carbamazepine is difficult to use in patients with other important comorbidities because it tends to interact with many medications. Despite having fewer side effects, oxcarbazepine can induce central nervous system depression or dose-related hyponatremia. (decreased sodium)
Patients vary widely in clinical response to either drug. The other can be moved to one to acquire a clearer answer. Warrier: ‘200mg of carbamazepine is as potent as 300mg of oxcarbazepine’ The impact of these drugs is notable on the control of paroxysmal pain
Lamotrigine
Lamotrigine is given as an adjunct for patients who show an adverse reaction to carbamazepine and oxcarbazepine. It tends to have less side effects than carbamazepine and oxcarbazepine
Gabapentin and pregabalin
In clinical application, gabapentin and pregabalin are shown to be less efficacious but lower in adverse effects than carbamazepine and oxcarbazepine. So, they may be used as an alternative to or in conjunction with carbamazepine or oxcarbazepine Although they are highly addictive.
Baclofen
Baclofen is especially useful in patients with a history of Multiple Sclerosis who may be treated with Baclofen for spasticity.
Botulinum toxin type A
Subcutaneous injection and injection of Botulin Toxin Type A over the gingival mucosa were found to significantly improve symptoms compared with placebo in a recent trial. Some of the mild adverse effects include transient facial edema and transient facial weakness.
Treatment of acute severe exacerbation
That is because in the case of severe exacerbations – these are the painful attacks that begin to occur more frequently, are more painful and the patient cannot even drink and eat. For short-course rehydration, maintenance of nutrition, and pain control, while optimizing long-term preventive treatment the patient would require hospital admission. However, opioids are used during such an episode but their effectiveness is debated. For immediate reduction of pain from these trigger zones, local anesthetic injections or topical lidocaine can be effective. Intravenous infusions of graded dosages of fosphenytoin (15mgs/kg over 30 minutes) and lidocaine (5mgs/kg over 60 minutes) while under cardiac monitoring are very efficacious.
Interventional treatments without Surgery
They are reserved for intractable pain resistant to medications. They can be divided into
- Needle-based Controlled Radiofrequency lesioning of the trigeminal ganglion.
- Trigeminoplasty: Cannonical Mechanical ballon compression of the trigeminal ganglion.
- Glycerol-based chemical rhizolysis
- Internal neurolysis – trigeminal nerve fascicle separation in the posterior fossa.
- Stereotactic Radiosurgery targeting the trigeminal root entry zone
Those patients who fail all of the above treatment methods are offered Microvascular decompression and we shall further discuss its surgical approach. The operating field is near the neurovascular structures, surgeon has to be careful. However, microvascular decompression has relatively superior outcomes in the elderly without co-morbidities compared to the younger population.